If anyone reading this is struggling or knows someone who is, know that you aren’t alone, and help is available. You can utilize the National Suicide Prevention Lifeline at
1 (800) 273-8255 or text HOME to 741741 to connect with the Crisis Text Line.
Executive Summary
As participants in a year-long Convergence dialogue, we advised on the strategies included in this report in service of our common goal—preventing firearm suicide. Convened as a cross-sector, cross-partisan group, we’ve forged trust, deepened mutual understanding, and identified solutions to address this urgent issue.
We come from a broad spectrum of backgrounds, perspectives and experiences. We come from rural and urban America. We hold a wide range of policy views. Our group includes individuals from gun rights and responsibilities advocacy groups, the gun industry, suicide prevention groups, gun violence prevention advocacy groups, mental health and medical practitioners, researchers, faith leaders, and those with a range of important personal connections to this issue. Among us are leaders and groups with opposing views and, in some cases, our organizations have not had meaningful, constructive interactions prior to this dialogue process. But we recognized America needs a different and better conversation on guns, and we are losing far too many of our friends and neighbors to suicide. In coming together, we sought to listen generously across differences, dig beneath top-line positions to understand underlying reasoning and motivations, and rely on both lived experience and data to find solutions.
Half of all suicides in recent years are by firearm.
CDC WISQARS
We hope this report can demonstrate:
- There are ideas and strategies we believe can meaningfully reduce the number of firearm suicides in our country—a project we agree is both urgent and doable.
- A civil, good faith conversation related to firearms is possible.
- Such a conversation can build empathy, understanding, and a deeper respect for one another even in the face of major disagreements.
Prior to starting this dialogue, Convergence conducted an assessment to determine where this process could add value, see what other good work could be learned from and built on, and find where the issue was “stuck” and in need of collaborative problem-solving. Convergence conducted over 130 interviews and small group discussions including people with widely divergent views and a mix of lived experience. We determined a better and different conversation was needed that meaningfully engaged a range of perspectives. Leaders right, left, center and apolitical in nature told us people needed time and space to build trust through a process devoid of standard issue talking points, out of the glare of political debates and inclusive of heterodox voices. As our assessment progressed and themes began emerging, we determined that a dialogue on preventing firearm suicide, the majority of gun deaths in the United States and on the rise over the past 20 years, held real potential for impact and was most achievable in this contentious issue space.

In the course of our research and ensuing dialogue we identified a set of shared facts the group could build upon. While the full report below includes a list of findings, we highlight some of those core facts here. While there was apparently a modest decrease in the total number of suicides in the United States in 2020, the trendline has been a roughly 35% increase since 1999. Of all the gun deaths in America each year, approximately 60% are suicides. Further, about half of all suicides in recent years are by firearm. For certain groups, the level of attempts and deaths by suicide is particularly concerning, including veterans and increasing rates for groups like African American youth/young adults, Native populations, and LGBTQ populations.
When it comes to guns and suicide, this group believes we’ve not collectively focused enough attention and scaled solutions that work to substantially move the numbers. Good work is happening and many programs are underway but much more can be done. Firearm suicides comprise the largest portion of gun deaths each year and yet do not get sufficient attention in the national conversation.
We believe it’s important that this group states loudly and clearly: suicide deaths by firearm are not inevitable. Suicidal ideation and periods of acute crisis are often short in duration and safe practices and well-constructed interventions can save lives. This report highlights a number of programs and interventions doing just that. Both message and messenger matter—we encourage all working on these issues to carefully consider language and we provide some guidance below on terms to use and avoid.
Of all the gun deaths in America each year, approximately 60% are suicides.
CDC WISQARS
All people benefit from attending to their mental health just as they do their physical health. We know suicide may result from a range of factors, including suffering from a mental health crisis. While gun owners are not more likely to experience a suicidal crisis than others, there is an elevated risk when such a crisis occurs. While a variety of means are used by individuals who die by suicide, the lethality is elevated when a firearm is used, with 83 – 90% of firearm suicide attempts resulting in death. Further, we know a suicidal person unable to access a gun does not typically find a different means and the acute period of crisis often passes. Therefore, means matter and that is why our group has focused specifically on a range of innovative ways to prevent firearm suicide. Evidence shows that heightened awareness, lethal means safety training, safe storage, and training of intervenors are some of the ways to prevent these deaths, as creating time and distance between a person in crisis and lethal means can save lives.
One of the themes from this dialogue was that both message and messenger matter in terms of effective prevention. While many individuals, professionals, and organizations have a role, we believe that gun owners must be an essential part of identifying, implementing, and promoting solutions that work. The inclusion of these voices in public health initiatives, programs, and research efforts to prevent firearm suicide can ground and will improve such efforts. Interventions that include a range of inputs, including the lived experience of gun owners, are critical to saving lives.
Our group sought not to stigmatize or blame but to build understanding among gun owners and non-gun owners, recognizing the individuals who comprise these groups include a wide range of cultural identifications and are hardly of one geography, gender, income group, race, sexual orientation, or identity. We cannot characterize either group with sweeping, simplistic terms or labels, especially as the demographic make-up of those choosing to own and not own guns continues to evolve and diversify.
83 - 90% of firearm suicide attempts result in death.
CDC WISQARS
Despite our many differences there is one fundamental truth: we all want to prevent firearm suicide and want any person struggling with suicidal ideation to receive competent care, support, and resources. We worked hard to avoid the pitfalls of well-worn debates that fall back on generalizations, which alienate those from differing backgrounds and perspectives. We discussed some statutory and regulatory actions to build understanding even when we couldn’t reach full agreement. We advised on several important strategies outlined in this report, as well as cautions about things that don’t work. They are summarized here:
- The possibility that a dialogue such as ours can be expanded, thus using the process that shaped and informed this group to engage others in a collaborative problem-solving approach.
- The findings and learnings, which include important data on lethal means, information on gun ownership, consideration of elevated or increasing suicide rates within certain populations and demographics, the importance of language and framing, and moving away from harmful and often incorrect stereotypes allowed participants to show up with their full and complex perspectives.
- Leading examples of best practices and promising programs, including grassroots efforts and innovative ways for gun owners to increase awareness, temporarily remove guns from their homes voluntarily, as well as models that promote and allow for safe storage practices.
- A call for increased funding, both public and philanthropic, that can prevent firearm suicide by supporting promising, innovative programs built on established principles and those with evidence-informed track records.
- A call for improvement and greater sophistication around evaluation of these programs, recognizing the complexity and difficulty of assessing prevention programs of many kinds, not just those focused on firearm suicide.
- Highlighting the work of a range of groups, especially in the firearms community, to expand their reach and scope through powerful and growing partnerships.
- A call for significant expansion of public and philanthropic research investments to study suicide, firearms, and suicide prevention strategies via partnerships with scientists, clinicians, consumers of mental health services, those with a range of lived experience, gun owners, and others.
- A call for new education campaigns around lethal means and suicide focused on credible messages and messengers, including work with a diverse mix of groups such as faith communities, affinity groups, doctors and mental health providers, and spaces utilized by gun owners to reach them with information on safety practices and how to access mental health resources. We want to bolster existing efforts and fill gaps to reach more people, including guidance on inclusive language to use and harmful practices to avoid.
We invite you to consider these ideas and take action in your own sphere of influence to save lives. We also invite leaders from the worlds of advocacy and policy, philanthropy, health care, community- and faith-based work, and other important sectors to recognize this type of collaborative problem-solving can lead to worthwhile, durable solutions. Join us in the work ahead as we seek to significantly reduce firearm suicide in the United States.
Convergence's Process
For years, leaders and citizens of diverse backgrounds approached us at Convergence about bringing our collaborative problem-solving approach to the issue of guns in America often highlighting the tangle of issues at play and a lack of clarity on how to improve on the contentious public conversation. Prior to starting this dialogue, Convergence conducted an assessment to determine where our process could add value, see what other good work could be learned from and built on, uncover tension points, and find where the issue was “stuck” and in need of collaborative problem-solving. Convergence conducted over 130 interviews and small group discussions including people with widely divergent views and a mix of lived experience. We learned when it comes to guns, there are no shortage of tension points, and quickly determined a better and different conversation was needed that meaningfully engaged a range of perspectives. Leaders right, left, center and apolitical in nature told us that people needed time and space to build trust through a process devoid of standard issue talking points, out of the glare of political debates focused on point-scoring, and inclusive of heterodox voices. As our assessment progressed and themes began emerging, we determined that a dialogue on preventing firearm suicide, the greatest source of gun deaths in the United States and on the rise over the past 20 years, held real potential for impact and was most achievable in this contentious issue space. Further, while we determined not to focus on other types of gun deaths for the scope of this dialogue, we also learned and recognized solutions that prevent suicide certainly can have other positive downstream effects.
While exploring this issue, Convergence staff learned that while a range of worthwhile efforts have emerged in recent years, they are not yet scaling up to meet the challenge. Innovative practitioners, gun community leaders, researchers, and medical experts agreed some initial foundational understanding of access to lethal means had been reached in recent years but that much more work was needed. Critically, those interviewed agreed that a space to build on that foundation with leaders from various sectors and ideological perspectives held value, though some were skeptical. Ultimately, those who agreed to participate in this dialogue saw particular value in a collaborative process to further act on the desire to save lives and an earnest hope to better understand the prerogatives and positions of those with whom they disagree. That said, a lack of trust and perceived bad faith were cited again and again as reasons why the existing national conversation was so difficult and ineffectual. For those close to communities of gun owners and for others not connected to them as deeply, a strong desire to center and understand gun owner motivations drove this work. Further, a recognition that gun owners are not monolithic, hold a wide range of views, and aren’t simply part of one “culture” would be critical to meaningfully grappling with behavior change and any emerging education efforts to prevent firearm suicide.
Coming into the dialogue, leaders from a range of perspectives felt caricatured and misunderstood. Self-described advocates with a particular focus on gun violence prevention sometimes felt their work was incorrectly described as having sinister motives or was disrespectful toward the rights of gun owners even as they worked to reduce injuries and prevent deaths by suicide. Gun rights advocates and other gun industry leaders felt their views were often oversimplified, that gun owners were reduced to stereotypes at times, and that they too wanted to prevent deaths and promote responsible practices. Years of unhelpful sound bites and overly broad labels used in all-or-nothing political debates dragged the national conversation to an acrimonious place; however, as mentioned, careful, quiet work in the field had led to some ability to better understand firearm suicide. More research and more willing leaders were needed to expand the reach of existing interventions and more trusted messengers to reach diverse populations. Our dialogue group hoped to fill some of those gaps but would of course need to build a base of trust, engage in shared learning, and bring a spirit of curiosity.
We conducted over 130 interviews and small group discussions.
Connections made in the dialogue meetings led to relationships outside.
Leaders from a range of perspectives felt caricatured and misunderstood.
Our dialogue group’s ability to stay together, build an arc of momentum, and eventually work toward sharing these strategies involved some key components. One was the commitment to listen generously, and another was taking care with and engaging in conversation about language around these topics, sometimes down to individual words. It was important to get underneath stated positions to understand motivations, which required asking genuine and open-ended questions with a real curiosity. Regarding divides over firearms, language was important as certain terms alienate people from a particular orientation. One person’s “accurate” description may seem incendiary to someone else, and we tried to hear each other and adopt more inclusive terms. This sometimes took multiple tries and patience. We also shared personal experiences, including losing people to firearm suicide, in an effort to not just show empathy but unpack what happened and what could have been done differently. While both an attempt and a death by suicide can create a crisis for the many people impacted, it also means many people and groups can help respond and intervene, including, for some, a reliance on faith leaders and, for others, mental health professionals and networks of support including family and friends.
A mix of clear-eyed analysis and vulnerability were both at play. Some in the group were less familiar with guns and expressed their lack of knowledge, while some raised the ways gun ownership has been viewed through a racialized lens and how all gun owners don’t receive the same deference and good faith assumptions. Others made clear labels like “gun control” and “weapons of war” and even “common sense solutions” can be off-putting and the importance of addressing people on terms that resonate for them. We also found a real desire to make the conversation about mental health care explicit and more sophisticated than often happens, including what competent care looks like that doesn’t cause gun owners to forego care out of fear and anxiety. Connections made in the dialogue meetings led to relationships outside, which allowed people to unpack tough issues and begin finding ways to collaborate.
Finally, learning together was crucial. Folks in the group and outside it with targeted expertise shared a host of information on suicide and firearms. Parts of the conversations were difficult, especially considering discussing suicide at all can be challenging and requires care and nuance with language. Along the way, we sometimes needed to regroup and try again after getting stuck. The momentum built over time came through repeated efforts to show curiosity, to give airtime even to issues where we couldn’t find agreement, and to think hard about how to drive behavior change and speak in the values of those we most desire to impact.
What We Learned
The group engaged in a wide range of shared learning – from breakdowns of firearm suicide data by demographics to understanding the complexities of gun ownership. Our two main learnings are that suicide rates differ across demographics and many intersectional identities; and, who owns guns and the reasons why they own guns, are equally as heterodox. There is stigma around seeking help and pervasive myths about what getting help will look like. All of this impacts the language, messengers, and messages that will be most effective at reducing firearm suicide.
Suicide Rates
Over the past 20 years, the United States has experienced increasing suicide rates. In 2019, the most recent year that data is available, 47,511 individuals died by suicide, making it the 10th leading cause of death in the U.S. While there was apparently a modest decrease in the total number of suicides in the United States in 2020, the trendline has been a roughly 35% increase since 1999.
Out of all the gun deaths in America each year, approximately 60% are suicides. Furthermore, of the 47,511 suicide deaths in 2019, approximately 50.4% were firearm suicides. While a range of means may be used in a suicide attempt, for fatal attempts, guns are statistically the most lethal with 90% of suicide attempts with a firearm resulting in death.
Gun owners are no more likely than non-gun owners to experience suicidal ideation. However, the presence of a firearm is an independent risk factor for all members of a household where a gun is present. And, 90% of individuals who attempt suicide and survive do not go on to die by suicide. Thus, the dramatic difference between these survival rates indicates that the suicide rate would decrease if we can reduce firearm suicides. That is why our group unequivocally supports the notion that means matter.
Rates and considerations across demographics
There are stark differences between demographic groups when it comes to suicide generally and methods more specifically. An important note on demographic differences in suicide is that individuals have intersectional identities. While we did our best to account for many of these overlaps, not all are captured.
Our group engaged in shared learning around how suicide rates differ among these various groups with the intention of creating a common base of knowledge and a reference point for thinking about strategies.
Overall Suicide Rate by Race (1999 - 2019)
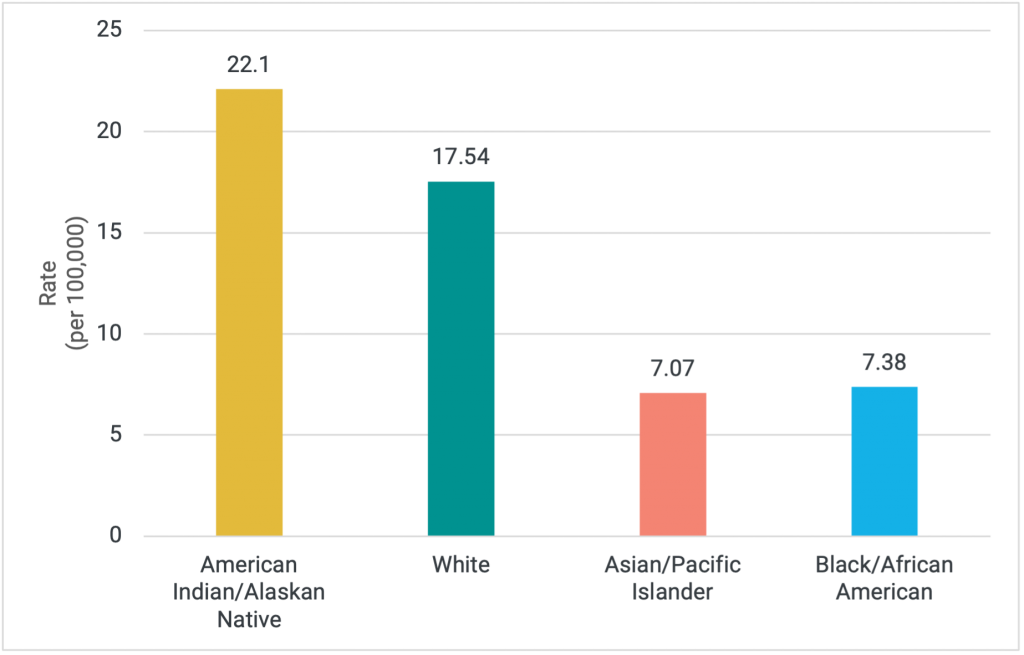
CDC WONDER
Firearm Suicide Rate by Race (1999 – 2019)
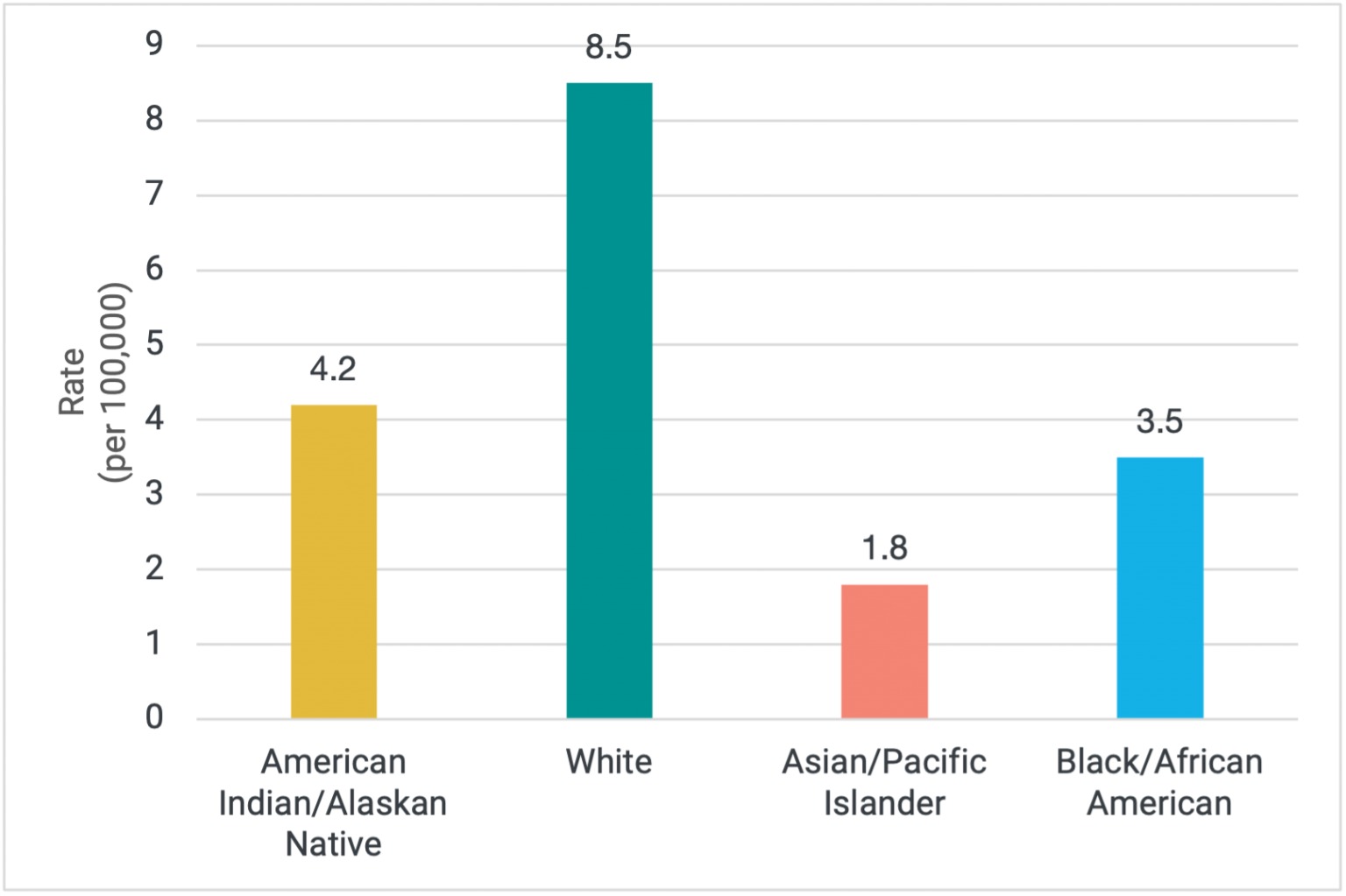
CDC WONDER
Race
Suicide rates are highest among American Indians/Alaskan Natives (22.1 per 100,000). Historically, the crude rate (meaning total number) for whites has followed American Indians/Alaskan Natives; however, suicide rates for other racial groups have been on the rise, particularly among young Black men. When rates are broken down by method, looking specifically at firearms, whites have the highest rate of suicide.
Whites
In 2019, the suicide rate among whites was 17.54 per 100,000. While suicides in the white community do not represent the highest crude rate of deaths, the age-adjusted rate places middle-aged white men at the top for overall suicides.
Furthermore, when the scope of suicides is narrowed to only firearm suicides, whites comprise the overwhelming majority of these suicides at approximately 85%.
American Indian & Alaskan Natives
It’s important to note that suicide data collection in American Indian and Alaskan Native (AI/AN) communities is complicated due to a number of factors, including historical racial misclassification as well as the overlap in governmental jurisdictions that these communities live under.
AI/AN communities experience the highest rates of suicide overall (22.2 per 100,000) as well as the highest suicide rate during adolescence and young adulthood, which is different from the national trend where the rate of suicide peaks mid-life.
Firearms are used at a rate of 4.2 per 100,000 within these communities. However, in some tribal communities the use of firearms is lower. There are likely cultural influences as to why this is the case, including in some Tribes that using a firearm frequently results in severe disfigurement and the cultural practice of viewing the deceased’s body and beliefs about the afterlife result in different lethal means being used.
African Americans
The suicide rate for African Americans overall is 7.4 per 100,000 making it less common compared to other demographic groups. The rate of firearm suicide for all ages is 3.5 per 100,000 within the African American community. However, both suicide attempts and deaths by suicide have substantially and persistently increased among Black adolescents since 1993.
Suicide is now the 10th leading cause of death among black 5- to 11-year-olds, where it used to be the 14th leading cause of death in 1993.
Both male and female adolescents (mean age is 16) who are black are 1.04 and 1.02 times more likely to attempt suicide than those who are not, respectively.
Age
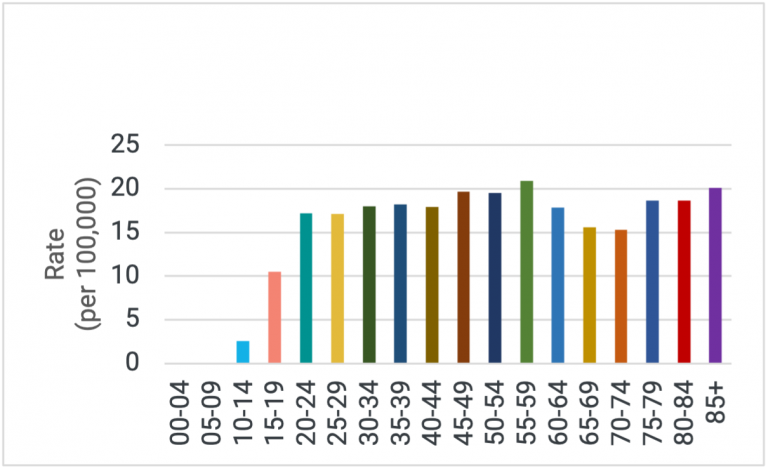
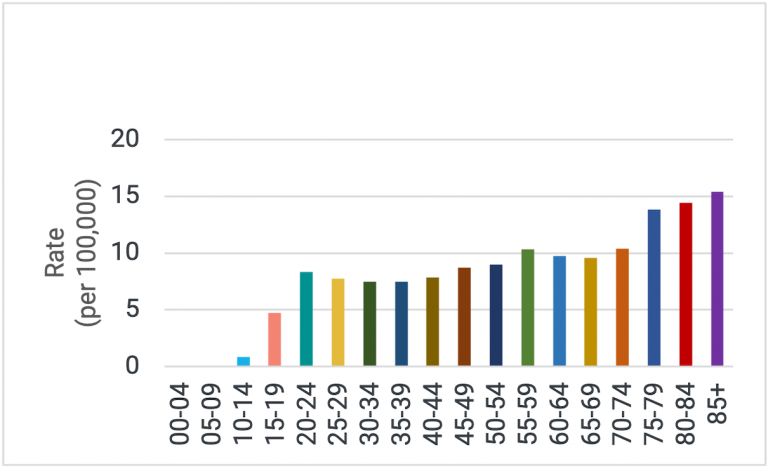
Suicide is not isolated among one age group. For individuals ages 10 – 34 it’s the second leading cause of death, the 4th for individuals ages 35 – 44, and the 5th for individuals ages 45-54 as of 2019. Despite suicide not being a leading cause of death among the general population of those aged 65+, males over 65 are drastically more likely to end their life using a firearm than females in the same age bracket (78% vs. 34% respectively).
Age-Adjusted Overall Suicide Rate (2019)
Age-Adjusted Firearm Suicide Rate (2019)
Gender and LGBTQ Status
Gender and LGBTQ status represent another important set of demographic factors to consider in the context of firearm suicide. There are strong differences in the rates of death by firearm suicide based on gender and within the LGBTQ community.
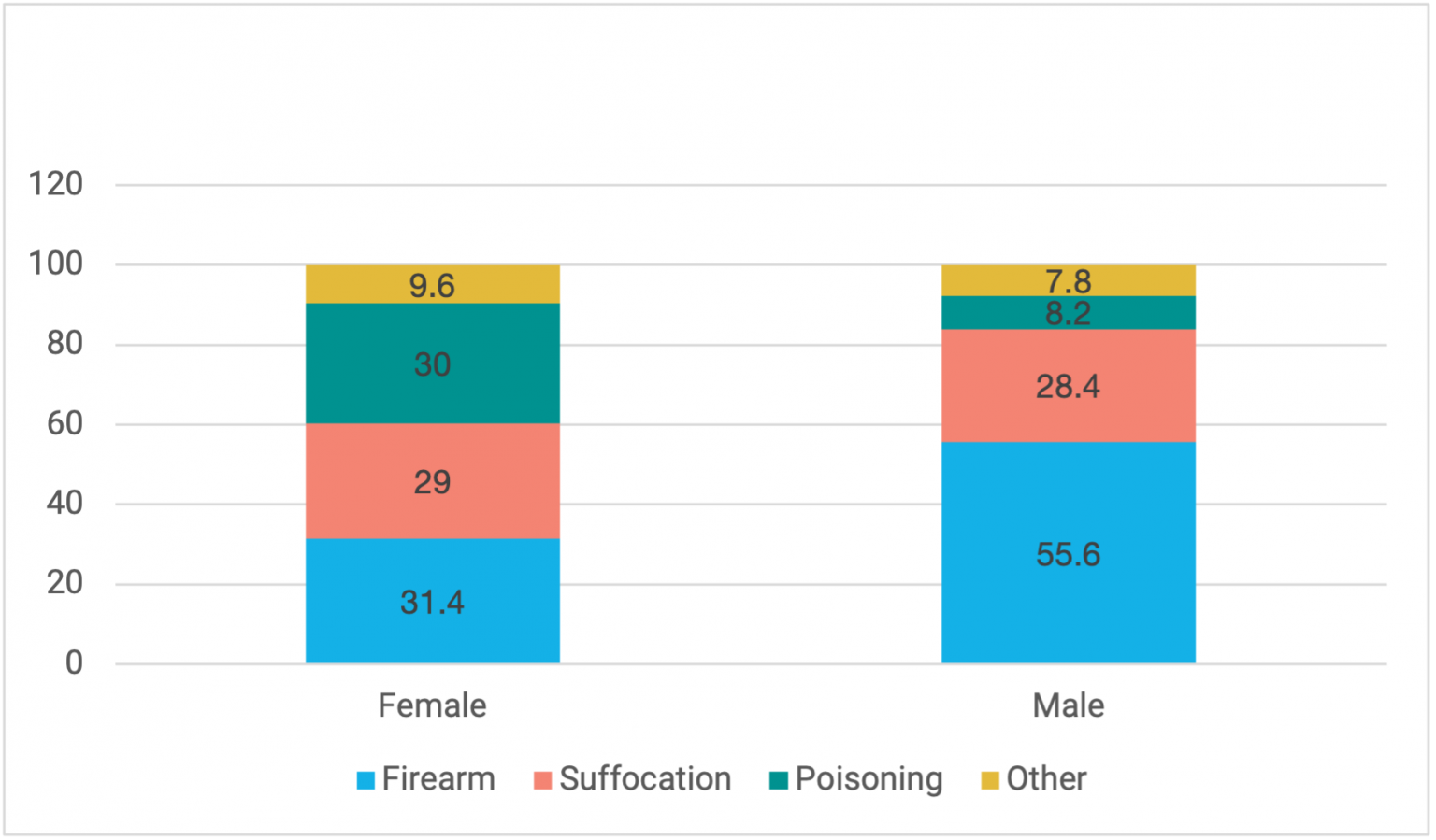
Male individuals have a much higher rate of suicide by any means than female individuals, dying by suicide at 3.63 times the rate. Furthermore, men are much more likely to use a gun than women (56% and 31%) respectively. While women are less likely to die by gun suicide than other means, the rate at which they use guns to die by suicide increases as they age.
The group also paid particular attention to the disparities that exist when comparing data on the LGBTQ community and their heterosexual, cisgender counterparts. Suicide attempts are four (4) times greater among LGBTQ youth than their heterosexual, cisgender counterparts. Less is known about how often members of the LGBTQ community die by suicide, and in particular firearm suicide, because data collection around gender identity and sexual orientation is either inadequate or simply not collected. It is important to note that the disparities that do exist should not be construed as causation – LGBTQ individuals are not more likely to attempt or die by suicide because of their identity or orientation – rather they experience other stressors that are risk factors for suicidal behavior, such as discrimination and family and social rejection. These experiences have the potential to increase negative mental health outcomes. Put simply, members of the LGBTQ community experience stressors their cisgender, heterosexual counterparts never experience.
Percentage of Suicide Deaths by Means & Gender (2019)
Veterans
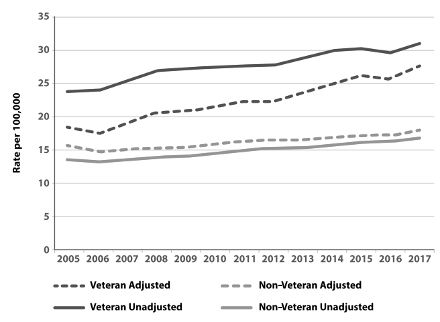
While the raw number of veteran suicides is significantly lower than the general population, veterans experience drastically higher rates of suicide than the non-veteran population: 31 per 100,000 for veterans and 17 per 100,000 for non-veterans. Furthermore, when broken down by gender, there is a divergence in suicide rates between male and female veterans. The rate of suicide among male veterans is 39.1 per 100,000 while female veterans experience a suicide rate of 16.8 per 100,000.
Firearm suicide accounts for the majority of suicide deaths among veterans. Approximately 69.4% of veteran suicide deaths involve a firearm.
Unadjusted and Age- and Sex-Adjusted Suicide Rates for Veterans and Non-Veteran Adults (2005–2017)
Gun ownership in the United States
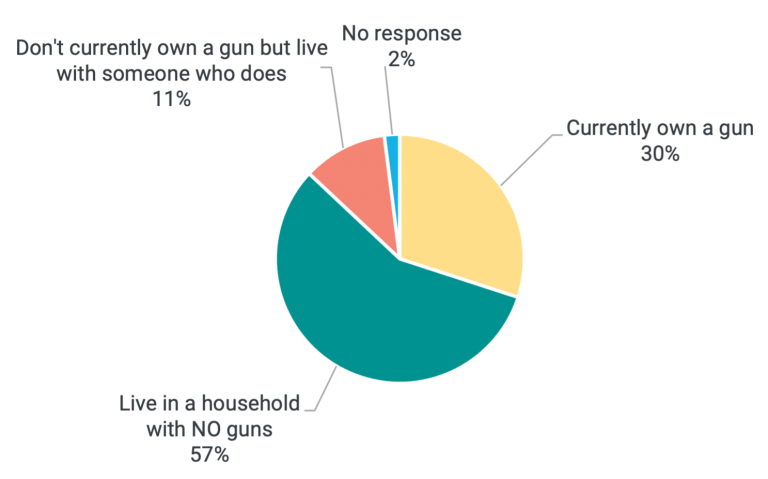
Gun owners are a diverse group across gender, age, geography, race, and other factors. Approximately four in ten adults in the U.S. live in a household with at least one gun present, according to this Pew data – though we know gun sales have broken records in recent years likely driving this number higher.
White adults are more likely than Black or Hispanic adults to own guns, and white men are particularly likely to be gun owners: 48% of white men say they currently own a gun, compared with 24% of white women and men of color and 16% of women of color. Even though predominant ownership is among middle-aged white males, ownership is changing, with more women and minority individuals purchasing firearms. Our group has seen anecdotal evidence of this trend and as mentioned above, we know gun purchases have climbed and broken records in recent years, which includes a mix of existing gun owners purchasing additional guns and new gun owners choosing to buy.
Gun owners are a diverse group across gender, age, geography, race, and other factors. Approximately four in ten adults in the U.S. live in a household with at least one gun present, according to this Pew data – though we know gun sales have broken records in recent years likely driving this number higher.
White adults are more likely than Black or Hispanic adults to own guns, and white men are particularly likely to be gun owners: 48% of white men say they currently own a gun, compared with 24% of white women and men of color and 16% of women of color. Even though predominant ownership is among middle-aged white males, ownership is changing, with more women and minority individuals purchasing firearms. Our group has seen anecdotal evidence of this trend and as mentioned above, we know gun purchases have climbed and broken records in recent years, which includes a mix of existing gun owners purchasing additional guns and new gun owners choosing to buy.
US Gun Ownership
Additionally, there are regional differences in firearm ownership. Individuals who reside in the Southern, Midwestern, or Western parts of the U.S. are more likely to own guns (36%, 32%, and 31% respectively) than those who live in the Northeast (only 16% report owning a gun). Furthermore, individuals who live in urban areas report that they are much less likely to own a gun than those who live in rural areas (28% versus 46%).
An important note – there are complex perceptions of gun ownership that are dependent on race, ethnicity, economics, and geography. We discussed how racial bias plays a role in perceptions of ownership in the African American community in particular. We also discussed how the method of acquiring a firearm differs, sometimes not through legal means, which impacts intervention methods and underlines the fact that our existing statistics may not fully capture the percentage of Americans regularly owning or using guns.
The motivations behind individual decisions to own a gun are multifaceted. There are a range of intended uses, including, but not limited to: personal safety/defensive uses, hunting, sports shooting, enjoyment, law enforcement jobs, as well as cultural traditions, political considerations, geographic location, and personal experiences that might make someone more likely to own a firearm. Because gun ownership and possession are sometimes tied to an individual’s sense of personal safety, communications and intervention techniques for suicide prevention are complicated. A person at-risk of suicide with access to lethal means like guns may view the gun as a last vestige of personal protection. This may be particularly true of veterans.
Although having a gun present in one’s home increases the risk of suicide death for anyone in the home (because of increased access to lethal means), individuals may not know this, feel it applies to them, or think this risk outweighs their other safety concerns. Assessment of an individual’s own risk is complex and difficult; there are growing efforts to include conversations about risk and safety into firearms training.
Language, framing, and the complexity of messaging
We spent some time together exploring the word choices we, our organizations, and our constituents use. Words matter tremendously in this contested arena. Words and phrases can be fraught and send signals of whether people are initially aligned or at odds before a conversation even starts. Thus, careful communication and messengers are essential to ensure outreach and advice are not only given but heard. Credible messengers and some effort at cultural competency are important for all involved. We explored a few of the following terms. More about word choice can be found in forthcoming publication by some members of our group.
Stigmas and Myths
We also explored stigmas and myths about these issues. Stigmas exist around seeking treatment for mental health issues, and myths exist regarding the impact on gun ownership if one seeks help, which can obscure the ultimate goal of making sure people receive quality and timely care.
Myth
Individuals with a diagnosed mental illness are the only ones who experience suicide and suicidal ideation.
Fact
Suicidal ideation can occur by anyone, whether or not they have a diagnosed mental health illness.
Myth
Suicide is inevitable.
Fact
Suicidal ideation and periods of acute crisis are often short in duration and interventions by the right people can save lives. Means matter precisely because a person who survives a suicide attempt typically does not go on to later die by suicide.
Myth
If an individual reveals they own guns to a mental health professional, they will be put on a no-buy list and have their guns confiscated.
Fact
Although laws differ from one state to the next, mental health providers don’t have the ability to place an individual directly on a no-buy list. In most cases, removal of firearms is temporary and carried out in a legal process where imminent danger appears likely. Mental health professionals and doctors can strengthen their ability to engage respectfully with gun owners by understanding their needs, values, and lived experience just as they seek to do so with other people to promote strong rapport and provide competent and individualized care.
Myth
Individuals with a diagnosed mental illness are the only ones who experience suicide and suicidal ideation.
Fact
Suicidal ideation can occur by anyone, whether or not they have a diagnosed mental health illness.
Myth
Suicide is inevitable.
Fact
Suicidal ideation and periods of acute crisis are often short in duration and interventions by the right people can save lives. Means matter precisely because a person who survives a suicide attempt typically does not go on to later die by suicide.
Myth
If an individual reveals they own guns to a mental health professional, they will be put on a no-buy list and have their guns confiscated.
Fact
Although laws differ from one state to the next, mental health providers don’t have the ability to place an individual directly on a no-buy list. In most cases, removal of firearms is temporary and carried out in a legal process where imminent danger appears likely. Mental health professionals and doctors can strengthen their ability to engage respectfully with gun owners by understanding their needs, values, and lived experience just as they seek to do so with other people to promote strong rapport and provide competent and individualized care.
Examples of Taking Action
Our group was comprised of many individuals and organizations already taking action on this topic. To learn from one another, we identified a range of programs that are seeking to effectively address suicide by firearms. These examples are included below.
- Walk the Talk America (WTTA) works to raise awareness and create a change in the misunderstandings regarding mental illness and firearms by bringing together industry leaders. They develop programs for suicide prevention, firearms negligence, trauma mitigation, and child safety. Their programs include classes to educate and improve mental health clinicians’ understanding of firearms culture; efforts to work with firearms manufacturers and gun shops to include information cards about mental health with the sale of any firearm or firearm accessories; and a campaign to encourage gun owners to surround their gun safes with reminders of what’s important in their life to cause a pause every time they go near their safe, whether in suicidal crisis or not.
- The Overwatch Project is building the equivalent of the “Friends Don’t Let Friends Drive Drunk” campaign for preventing veteran suicide, only instead of talking about alcohol and vehicles, they focus on firearms and suicide.
- Gun Shop Projects, now present in many states, build on partnerships between firearms retailers, ranges, and clubs and public health experts. They provide retailers, instructors, and customers of all experience levels with firearm suicide prevention educational materials.
- The American Foundation for Suicide Prevention —National Shooting Sports
Foundation Suicide Prevention Program is a partnership that was founded in 2016 to allow for both organizations to embark on a first-of-its-kind national plan to build and implement public education resources for firearms retailers, shooting ranges and the firearms-owning community about suicide prevention and firearms.
- Project 2025 is a nationwide initiative housed within the American Foundation for Suicide Prevention to reduce the annual rate of suicide in the U.S. 20 percent by 2025. Project 2025 is working with key partners to educate the range, retail, and broader firearms-owning communities on how to spot suicide risk and know what steps they can take to save lives.
- Counseling on Access to Lethal Means (CALM) is a course about how to reduce access to the methods people use to die by suicide. It covers who needs lethal means counseling and how to work with people at risk for suicide—and their families—to reduce access.
- Lock to Live is a free online tool to help adults make decisions about temporarily reducing access to potentially dangerous things, like firearms, medicines, sharp objects, or other household items.
- The Trevor Project is the world’s largest suicide prevention and crisis intervention organization for LGBTQ (lesbian, gay, bisexual, transgender, queer, and questioning) young people. They provide various trainings, including, a free online learning module with a video, curriculum, and teacher resources for middle school and high school classrooms; a training course that introduces adults to suicide prevention techniques based on Trevor’s CARE model (Connect, Accept, Respond, Empower); and, a training that introduces adults to the unique needs of LGBTQ youth.
- Celebrating Life Suicide Surveillance System was developed based on a decade of mounting concern over increasing youth suicide. The White Mountain Apache Tribe (WMAT) passed a tribal law mandating that any suicidal incident occurring on tribal lands—including ideation, attempts, deaths, and non-suicidal self-injury—be recorded into a tribal suicide surveillance system. The White Mountain Apache tribe saw a 38% reduction in suicides overall between 2007-2012.
- Help Alleviate Valley Experiences Now (HAVEN) trains congregants to recognize warning signs of depression and anxiety; works with clergy members to incorporate messages about mental health and help-seeking into Bible study lessons, Sunday school classes and sermons; and aids churches in developing mental health resource directories.
- The Center for Guns Rights and Responsibilities (CGRR) seeks to exemplify and promote a new conversation about guns in America. CGRR insists on respecting everyone’s perspective, whether a gun owner or not, while working to protect both individual gun rights and lives. CGRR’s GunPRO is an initiative to have gun owners voluntarily sign on to principles of gun ownership. GunPRO plans to focus on encouraging gun owners to commit to get Education and training in the responsible and safe use of the firearm(s); take steps to prevent unauthorized access to their firearms; and, seek help and remove access to firearms during times of extreme emotional stress or mental illness that could impair their judgement in regard to responsible use. These commitments are witnessed by two peers invited by an individual purchaser who will both commit to supporting the purchaser in those commitments.
- Hold My Guns works within the firearms community, combined with appropriate community partner alliances, to raise awareness and promote a self-governance, non-legislative approach to addressing the prevention of suicide, theft, and accidental shootings. They encourage educational and enrichment opportunities that approach stressors contributing to suicide risk in a way that is matter of fact, helpful, and in the stigma-free environment of partnering gun shops.
Strategies for the Future
1
Increase and expand funding for programs and their subsequent evaluation that seek to prevent suicides by firearm.
- We need greater funding for programs and initiatives focused on firearm suicide prevention. We recognize public funding may be limited to initiatives with a long-established track record. We hope that private, philanthropic funders will consider the below guidance in their work to support firearm suicide prevention efforts:
Explicitly emphasize the importance of funding efforts that address the lethality associated with firearms as a method;
Include engagement with, input from, and co-creation, where possible, by gun owners from the outset, as well as others with key lived experience, in order to consider the population these efforts aim to most directly impact. We also encourage funders to support partnerships between unlikely allies, where constructive.
Further, we encourage funders, whatever their particular views on gun policy, to broaden the kinds of programs and organizations which they fund.
Too often, the debate on public policy has left funders with a limited range of allied grantees, which in turn reduces our collective ability to bring diverse groups with important knowledge together to jointly seek to solve this problem. We believe that this issue is too important and urgent to not work together, even when some areas of strong disagreement remain. Innovative programmatic efforts to prevent firearm suicide merit consideration even when those running such programs may not be aligned with 100% of funder priorities on public policy.
- We believe funding should cover both promising, innovative efforts built on established principles as well as those with strong evidence-informed track records. This means newer, grassroots efforts rooted in best practices may merit consideration to help them build an evidence base recognizing rigorous evaluation takes significant investment not always available to smaller initiatives. Evaluation of this work and any risk prevention effort is inherently challenging. We need more and better data and a recognition that clarifying which factor or intervention saved a life is quite difficult.
2
Highlight current work by firearms groups and others to promote and expand their suicide prevention reach and scope.
- We recognize the strong existing and emerging work currently being done both outside and inside the firearm community by gun industry and gun community leadership. There are lessons to be learned from these efforts as we call for even more urgent action. This report cites several initiatives our participants either lead or know about.
- We support, encourage, and want to incentivize gun owners, gun rights groups, and the gun industry to be outspoken in ways that strategically drive behavior change to prevent firearm suicide. We particularly call for efforts that use inclusive language, connect with the values of gun owners, and aim to empower. We want to further normalize safety practices and behaviors that many gun owners already employ so they are more widespread, and ideally universal, when it comes to storage practices.
- We call on leaders to build unique partnerships to drive change (an example is the AFSP and NSSF partnership described above) and elevate efforts that people and groups outside of the gun community can be a part of to make a positive impact as well. We all have a part to play.
- We believe in promoting safer in-home and voluntary out-of-home storage opportunities, consistent with state and local laws, to reduce firearm access to individuals at-risk of suicide. Temporarily limiting access to lethal means is critical to preventing firearm suicide.
3
Increase and expand firearm suicide prevention research.
- We encourage funders, public and philanthropic, to study suicide, firearms, and suicide prevention strategies via partnerships with scientists, clinicians, consumers of mental health services, those with a range of lived experience, gun owner-aligned groups, and others.
- We challenge more funders to enter this space beyond those already involved. We particularly promote research efforts that “improve [our] understanding of the determinants of firearm injury, the identification of those at risk of firearm injury […], the development and piloting of innovative interventions to prevent firearm injury and mortality, and the examination of approaches to improve the implementation of existing, evidence-based interventions to prevent firearm injury and mortality.” Specific focus areas for increased understanding should include, but are not limited to:
diverse populations and risk with a focus on equity that contextualizes firearm suicide and gun ownership,
the language and science of persuasion around personal safety and suicide,
mental health stigmatization among key populations like gun owners and how to overcome it,
co-produced research with gun owners and advocates, and
research into efforts that lead to improved or new programs and thus reduced rates of firearm suicide.
4
Amplify education on lethal means and suicide prevention to drastically reduce the number of firearm suicides in the United States.
- We call for education campaigns, including bolstering existing efforts and filling gaps, that do a range of things, including taking account of the complex perceptions of gun ownership that are often dependent on race and ethnicity. These campaigns should include:
Specific calls to action for targeted audiences.
Credible messengers to deliver campaign messages that authentically resonate with the values of the intended audience.
The best expertise in communications science to expand awareness and drive behavior change about guns and suicide.
An acknowledgement of the differing means of firearm acquisition, sometimes through non-traditional methods, which will impact interventions.
- We call on diverse leaders to share existing program information to expand their reach and scale by:
Identifying channels to deliver existing program information across interests and value groups—faith communities, neighborhood groups, affinity groups, spaces utilized by gun owners, and others.
Clarify the roles leaders in these spaces can constructively play.
Deliver existing program information to gun owners and non-gun owners on the importance of interventions due to lethality of firearms when used in suicide attempts and how to get mental health support.
- We seek to provide information on our findings to legislators, including those who can impact research and funding.
- Many doctors and mental and behavioral health care providers offer high quality care to a range of populations. We call for an increase in training and competency regarding treatment for those with suicidal ideation and access to guns following best practices so that firearm owners don’t forego care.
5
Demonstrate that dialogue can occur to rebuild trust, forge stronger mutual understanding, find common ground, and take action to prevent firearm suicide.
- We will model a different and better conversation about guns in America through public-facing events and an innovative range of communication vehicles reaching diverse audiences. We invite others to join us.
- We will leverage our own unique networks to tell the story of this dialogue to different types of audiences and promote the specific ideas included here to prevent firearm suicide. Recognizing others possess good ideas and valuable insights, we invite people from across sectors and backgrounds to join us, engage in your own constructive efforts, and work together to prevent these deaths.
Who We Are
Convergence Dialogue on Guns and Suicide Prevention Participants
Dr. Emmy Betz
Firearm Injury Prevention Initiative,
University of Colorado
Anschutz Medical Campus
Bill Brassard
National Shooting Sports Foundation
Chris Cheng
The History Channel’s Top Shot
Season 4 Champion
Elaine Frank
Counseling on Access to Lethal Means,
Dartmouth College
Jennifer Hoppe
Everytown for Gun Safety
Dr. Doreen Marshall
American Foundation for Suicide Prevention
Dr. Megan McCarthy
Rev. Dr. Sherry Molock
George Washington University,
Department of Psychological & Brain Sciences
Casey Pick
The Trevor Project
Rob Pincus
Second Amendment Organization
Dr. Rajeev Ramchand
RAND
Rev. Margery Rossi
Gun Violence Prevention Group,
Presbyterian Peace Fellowship
Peter Sargent
Backstop
Responsible Gun Owners
Mike Sodini
Walk the Talk America
The stakeholders listed participated in a year-long Convergence Dialogue to engage in shared learning and consider and advise on strategies they individually believe can contribute to preventing firearm suicide. Organizational affiliations are listed for informational purposes only and to demonstrate the breadth of perspectives represented. Participation in this process is neither an endorsement of other participants’ organizational policies or public positions nor of any or all specific strategies included. Leaders across sectors and backgrounds are asked to consider these strategies and to take action on those they believe will help reduce suicide by firearm.
Convergence Dialogue on Guns and Suicide Prevention Project Staff and Consultants
David Eisner, President and CEO, Convergence
Russell Krumnow, Senior Director of Projects, Convergence
Erica Loken, Projects Associate, Convergence
Patrick Field, Senior Mediator, Consensus Building Institute
Design by Alexandra Chugunova Frazier, Communications Assistant, Convergence
Download
Sources
Ahmad, F. B., & Anderson, R. N. (2021). The leading causes of death in the us for 2020. JAMA, 325(18), 1829. https://tinyurl.com/AhmadAnderson.
Attempters’ Longterm Survival. (2013, January 9). Harvard School of Public Health. https://tinyurl.com/longtermsurvival.
Black Populations. Suicide Prevention Resource Center. Retrieved from https://tinyurl.com/blackpopulations.
CDC WISQARS Fatal Injury Reports, National, Regional and State, 1999 – 2019. https://tinyurl.com/CDCWISQARS.
Conner, A., Azrael, D., & Miller, M. (2019). Suicide Case-Fatality Rates in the United States, 2007 to 2014. Annals of Internal Medicine, 171(12). https://tinyurl.com/ConnorAzraelMiller.
DeSilver, D. (2013, May 24). Suicides account for most gun deaths. Pew Research Center. Retrieved from https://tinyurl.com/DrewDeSilver.
Fatal Injury Data Visualization Explore. (2001–2019). [Dataset]. Centers for Disease Control and Prevention. https://tinyurl.com/WIQARSVisualization.
Firearm Access is a Risk Factor for Suicide. (2017, January 6). Harvard School of Public Health. https://tinyurl.com/MeansMatter.
Firearm Injury and Mortality Prevention Research (R21/R33 Clinical Trial Optional). (2021). Department of Health and Human Services. https://tinyurl.com/GrantReference.
Haas, A. P., & Lane, A. (2015). Collecting Sexual Orientation and Gender Identity Data in Suicide and Other Violent Deaths: A Step Towards Identifying and Addressing LGBT Mortality Disparities. LGBT Health, 2(1), 84-87. https://tinyurl.com/HaasLane.
Hedegaard, H., Curtin, S. C., & Warner, M. (2021). Suicide Mortality in the United States, 1999¬-2019. National. Center for Health Statistics. https://tinyurl.com/HedegaardCurtinWarner.
Holliday-Moore, R. (2019, July 23). Alarming Suicide Trends in African American Children: An Urgent Issue. https://tinyurl.com/Holliday-Moore.
Igielnik, R., & Brown, A. (2017, June 22). Key takeaways on Americans’ views of guns and gun ownership. Pew Research Center. https://tinyurl.com/IgielnikBrown.
Ilgen, M. A., K. Zivin, R. J. McCammon, and M. Valenstein, “Mental Illness, Previous Suicidality, and Access to Guns in the United States,” Psychiatric Services, Vol. 59, No. 2, 2008, pp. 198–200. https://tinyurl.com/IlgenEtAl.
Leading Causes of Death Reports, 1981 – 2019. (1981–2019). [Dataset]. Centers for Disease Control and Prevention. https://tinyurl.com/LeadingCauses1.
Lindsey, M. A., Sheftall, A. H., Xiao, Y., & Joe, S. (2019). Trends of Suicidal Behaviors Among High School Students in the United States: 1991–2017. Pediatrics: Official Journal of the American Academy of Pediatrics, 144(5). https://tinyurl.com/LindseyEtAl.
Means of Suicide. (2021). Suicide Prevention Resource Center. https://tinyurl.com/MeansOfSuicide.
National Survey on LGBTQ Youth Mental Health 2021. The Trevor Project. (2021). https://tinyurl.com/TrevorProject1.
Office of Mental Health and Suicide Prevention, U.S. Department of Veterans Affairs. (2019). 2019 National Veteran Suicide Prevention Annual Report. https://tinyurl.com/VeteranSuicideReport.
Racial and ethnic disparities. Suicide Prevention Resource Center. Retrieved from https://tinyurl.com/Disparities1.
Stone, D. M., Jones, C. M., & Mack, K. A. (2021, February). Morbidity and Mortality Weekly Report: Changes in Suicide Rates — United States, 2018–2019 (70(8);261-268). Centers for Disease Control and Prevention. https://tinyurl.com/StoneEtAl.
Suicide statistics. (2021). American Foundation for Suicide Prevention. https://tinyurl.com/SuicideStats1.
Suicide Statistics. (2021). National Institute of Mental Health. https://tinyurl.com/SuicideStats2.
The Trevor Project: American Indian and Alaskan Native LGBTQ Youth Suicide Risk (November 2020): https://tinyurl.com/AIANPopulations.
Underlying Cause of Death, 1999–2019 Request. (1999–2019). [Dataset]. Centers for Disease Control and Prevention WONDER Database. https://tinyurl.com/WONDERCDC.
Convergence Center for Policy Resolution is a national non-profit based in Washington, DC that convenes individuals and organizations with divergent views to build trust, identify solutions, and form alliances for action on issues of critical public concern. Reports and recommendations issued under our auspices reflect the views of the individuals and organizations who put the ideas forward. Convergence itself remains neutral and does not endorse or take positions on recommendations of its stakeholders.
Convergence Center for Policy Resolution
1133 19th Street NW, Suite 410
Washington, DC | 20036
202 830 2310
www.convergencepolicy.org
© 2021 Convergence Center for Policy Resolution
Reproduction of all or part of this publication may be authorized only with consent and acknowledgment of the source.